Association between characteristics of swallowing-related muscles and trunk muscle mass - Scientific Reports
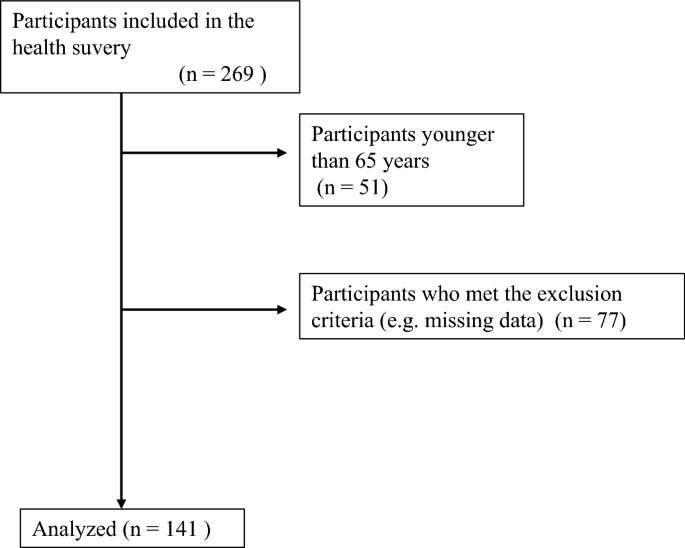
Swallowing function is associated with systemic factors. Whether trunk or appendicular skeletal muscle mass is a better indicator of swallowing-related muscle characteristics in community-dwelling older adults is not clear. Hence, we investigated the association between the characteristics of swallowing-related muscles (e.g., mass and quality) and trunk muscle mass. Community-dwelling older adults aged ≥ 65 years (n = 141; men: n = 45, women: n = 96) were recruited for this cross-sectional observational study via a health survey conducted in 2018. Trunk muscle mass index (TMI) and appendicular skeletal muscle mass index (SMI) were measured using bioelectrical impedance analysis. Cross-sectional areas (CSAs) and echo intensity (EI) of the geniohyoid muscle (GHM) and tongue were evaluated using an ultrasonic diagnostic apparatus. Multiple regression analysis was used to examine the relationship of the characteristics of swallowing-related muscle with TMI and SMI. Multiple regression analysis showed that CSA of the GHM was positively associated with both TMI (B = 24.9, p < 0.001) and SMI (B = 13.7, p = 0.002). EIs of swallowing-related muscles were not associated with TMI and SMI. Trunk muscle mass was associated with swallowing-related muscle mass and not muscle quality. The results of this study shed light on the elucidation of association of dysphagia with TMI and SMI. A health survey conducted in 2018 in Japan revealed the association between characteristics of swallowing-related muscles and trunk muscle mass. Participants aged between 65 and 65 years were recruited to participate in the study, which included those with a history of diseases affecting the muscles, obvious dysphagia, and missing relevant data. The study was approved by the Ethics Committee of the Tokyo Medical and Dental University and complied with the current ethical laws of Japan. Body mass index was calculated by dividing body weight by height squared, while Malnutrition was assessed using the MNA-SF18, with scores ranging as 0–2 or 0–3. The CSA of the swallowing related muscles was used as the proxy for swallowing- related muscle mass, and the range of interest was set to include as much muscle as possible. To avoid any correlation between these two conditions, the results were compared using Pearson’s Spearman and To-square tests.
Published : 2 years ago by Haruka, Japan, Tokyo Medical, Chantaramanee, Kanako, Ariya, Nakagawa, Ayako, Yamaguchi, Kohei, Yoshimi, Tohara, Thailand, Department of Preventive Dentistry, Nakane, Dental University, Ishii, Mueang Phitsanulok, Department of Dysphagia Rehabilitation, Naresuan University, Tokyo, Hasegawa, Shohei, Miki, Kazuharu in Lifestyle
The participants of a health survey conducted in 2018 in Japan were recruited for this study. Older adults aged ≥ 65 years who could perform activities of daily living independently and were able to follow instructions were included. Those with a history of diseases affecting the muscles (e.g., neuromuscular disease and cerebrovascular disorder with paralysis), obvious dysphagia (e.g., symptoms of severe aspiration after surgery for head and neck tumors), a pacemaker, or missing relevant data were excluded. Some of the data analyzed in this study have been reported in previous studies9,17, except for the data related to Eating Assessment Tool-10 (EAT-10) and the Mini Nutritional Assessment-Short Form (MNA-SF). The sample size for this research was determined by calculating the detection power of multiple regression analysis using G power 3.1 (Kiel University, Kiel, Germany). In the post hoc test, α was 0.05, effect size was f2, and the number of participants was 141. All analyses showed a high detection power of ≥ 0.95. After providing sufficient written and oral explanation, written consent was obtained from each participant. This study was approved by the Ethics Committee of the Tokyo Medical and Dental University (ref: D2014-047), and the study protocol complied with the current ethical laws of Japan.
Body mass index was calculated by dividing body weight by height squared. Muscle mass was measured by direct segmental multifrequency bioelectrical impedance analysis, using In Body S10 (InBody Japan, Tokyo, Japan), at five measurement sites on the trunk and left and right limbs. The InBody S10 device measures impedance using a multifrequency alternating current of 1, 5, 50, 250, 500, and 1000 kHz, with eight electrodes attached to the left and right limbs. At the time of measurement, each participant sat on a chair in a relaxed state, with the back not hunched against the backrest, hands lowered away from the trunk, and knees not bent at right angles but extended slightly forward12. The trunk muscle mass index (TMI) was calculated by dividing the trunk muscle mass by square of the height12. The appendicular skeletal muscle mass index (SMI) was calculated by dividing the total muscle mass of the limbs by square of the height. Malnutrition was assessed using the MNA-SF18, which consists of six questions, with scores ranging as 0–2 or 0–3. A score of 0 indicates the worst condition; the higher the score, the better the condition. With a total of 14 points, 12–14, 8–11, and 0–7 points indicate good nutrition, malnutrition risk, and malnutrition, respectively.
Tooth loss was evaluated by experienced dentists or dental hygienists and classified according to the Eichner classification19. Ultrasonography of the GHM and tongue was performed using an ultrasonic diagnostic apparatus (Sonosite M-Turbo; Fujifilm, Tokyo, Japan). All measurements were performed by an experienced dentist. A 2–5-MHz convex probe with a depth of 9.2 cm was used. At the time of measurement, the probe was covered with a water-soluble transmission gel, and the participant was seated facing forward. The frequency and depth were constant for all measurements. The probe was placed at the line connecting the left and right second premolars, perpendicular to the Frankfurt plane9. Ultrasonographic images were analyzed using ImageJ software (version 1.49; National Institutes of Health, Bethesda, MD, USA). The CSA of the swallowing-related muscles was used as the proxy for swallowing-related muscle mass. Echo intensity (EI) was measured as an indicator of muscle quantity. The range of interest was set to include as much muscle as possible, without including the fascia. The average of two measurements was used as the measured value. Previous studies have shown sufficiently high intrarater reliability of ultrasonography for the GHM and tongue9. The EAT-10 is a self-reported questionnaire for dysphagia and consists of 10 questions, with points ranging from 0 to 4. Dysphagia is suspected when the total score is more than 320.
The normality of each item was confirmed using the Shapiro–Wilk test. T-test, Mann–Whitney test, and chi-square test were used for comparing the data between men and women. Further, participants were classified into low or high TMI and SMI groups by sex, using the 1st quartile of TMI and cut-off value determined by the Asian Working Group for Sarcopenia, respectively21. Coefficients of the correlations of the characteristics of swallowing-related muscles with TMI and SMI were calculated using the Pearson’s and Spearman’s correlation tests for parametric and non-parametric variables, respectively. To examine the relationship of the characteristics of swallowing-related muscles with TMI and SMI, multiple regression analysis was performed using swallowing-related muscle characteristics as dependent variables. The explanatory variables were age, sex, tooth loss, MNA-SF points, EAT-10 score, TMI, and SMI. The categorical variables were sex (0, men and 1, women) and tooth loss (1, Eichner A; 2, Eichner B; and 3, Eichner C). The forced input method was selected as the input method. To avoid multicollinearity, we checked whether the variance inflation factor was < 10.
Topics: Fitness